
A lot of guys assume that if two products both say “testosterone” on the label, the price difference just comes down to marketing markup. That’s not what was actually happening when a guy I lift with, let’s call him Marcus because that’s not his name, cornered me by the water fountain a few months back with his phone out. Two tabs open. One was a telehealth clinic quoting him a supervised protocol with bloodwork attached. The other was a vial marked “not for human consumption,” priced at maybe a third of the cost. Same word printed on both screens. Testosterone. He wanted to know if he was about to find a smart deal or step on a rake.
I didn’t have a clean answer for him that day, so I went and did the reading I should have already done. Here’s the thing: I want to walk you through what I found before I tell you who I’d actually trust with this, because most of what gets written about testosterone skips the evidence part entirely and jumps straight to a coupon. That’s backwards. Let me be straight with you about what’s real first.
What this is actually for
Peel back the ads and the podcast-bro talk, and testosterone replacement therapy exists to treat one specific thing: hypogonadism, which is just a fancy word for a body that’s stopped making enough of its own testosterone. Usually it’s an injectable, cypionate or enanthate, sometimes a gel or cream, and often it travels with a sidekick medication, HCG or gonadorelin to protect fertility, or a SERM like enclomiphene for guys who’d rather nudge their own production up instead of replacing it outright.
Here’s the part that stopped me cold. The Endocrine Society’s 2018 clinical guideline says, in no uncertain terms, that this diagnosis belongs only to men who have both the symptoms and consistently, unequivocally low testosterone on a repeated fasting morning blood test, not just one number that happened to look low [1]. That’s not red tape for its own sake. It’s the line between a man who genuinely needs this and a tired guy who doesn’t. And it’s the first thing the research-site vial simply cannot offer, because there’s nobody on the other end of that transaction to run the test.
So before we even get to “approved versus compounded,” there’s a more basic fork in the road: one path starts with a diagnosis, the other starts with a checkout button.
Three things wearing one name
FDA-approved testosterone is the finished product, brand or generic, made to a federal standard, tested for safety and quality, handed over at a pharmacy with your name on the label. The recognizable injectable cypionate, the brand gels. The tradeoff is cost and rigidity: brand topicals especially can get pricey, and you’re stuck with whatever strength the manufacturer decided to make.
Compounded testosterone is still a real prescription, still ordered by a clinician, but prepared specifically for you by a licensed compounding pharmacy (typically what’s called a 503A pharmacy, working to USP standards). People go this route because it’s usually more affordable and because a compounder can build a concentration or a combination a boxed product just doesn’t offer. What stays intact is the whole point of medicine: someone diagnosed you, someone licensed is preparing it, and someone’s checking your labs down the road.
Research-grade testosterone isn’t a third medical option at all. It’s a different animal wearing the same name tag. It’s sold “for research use only,” meaning explicitly not for a human body, nobody screened you, nobody set your dose, and nobody stands behind what’s actually in that vial. The label might say testosterone. The accountability is zero. No diagnosis, no pharmacy standard, no one to call if your bloodwork goes sideways.
Marcus was about to treat these like three price points on one shelf. They’re not. Two of them are medicine. One is a chemical sold with a legal disclaimer telling you not to do the exact thing you’d be doing.
Three gates, and what happens when you skip them
The way I’ve come to think about it, legitimate testosterone therapy passes through three gates before it ever reaches your body: a diagnosis gate, a pharmacy gate, and a monitoring gate. The research vial skips all three, and that’s really the whole story in miniature. Worth keeping that frame in your head as you read what the actual trials found, because the trials only mean what they mean if those gates stayed shut behind them.
The best evidence we have on older men is the Testosterone Trials, a coordinated set of placebo-controlled studies in 790 men aged 65 and up with confirmed low testosterone, published in the New England Journal of Medicine in 2016 [2]. The wins were real and specific: meaningfully better sexual activity, desire, and erectile function compared to placebo, plus a modest bump in mood.
But here’s the honest part, the part the gray-market sellers would rather you not read twice. In that same trial, testosterone showed no significant benefit for vitality on a standard fatigue scale [2]. Read that again. If you’re buying testosterone hoping to feel like you did at twenty-five, in the best trial we’ve got, on men who genuinely qualified, it didn’t move the needle on energy. That’s true no matter which of the three tabs you buy it from.
Then there’s the heart question, which hung over this drug for a decade. TRAVERSE, published in NEJM in 2023, followed 5,246 hypogonadal men aged 45 to 80 who already had cardiovascular disease or a high risk of it [3]. The headline finding was reassuring: testosterone was noninferior to placebo for major cardiac events, 7.0 percent versus 7.3 percent.
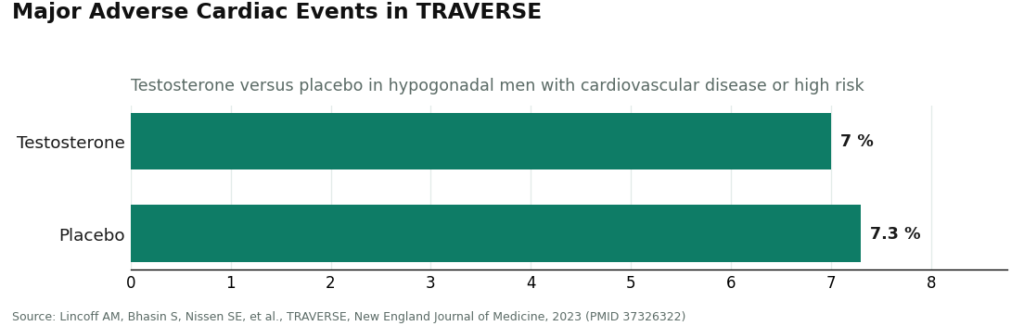
But TRAVERSE also turned up higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [3]. That’s not a reason to avoid this treatment if you actually need it. It’s exactly the kind of signal a supervising clinician exists to watch for. And it’s the whole argument against the research vial in one sentence: the reassuring numbers from TRAVERSE come bundled with monitoring. Take the monitoring away and you’re left holding the risks with none of the net underneath them.
So which door do you actually walk through
If you want the audited, federally reviewed product and the cost doesn’t bother you, FDA-approved testosterone through a real prescriber is a fine, uncomplicated choice. Nothing outranks it on regulatory pedigree.
If you want supervised care at a friendlier price, or you need a concentration or combination a boxed product doesn’t make, compounded testosterone through a licensed pharmacy is the natural fit, monitoring included, FDA caveat understood and out in the open. A lot of good telehealth care runs on exactly this model, and done right it carries the same safety net that made TRAVERSE’s numbers reassuring in the first place.
The research vial isn’t a cheaper version of either. It’s what’s left when you strip out the diagnosis the guideline requires [1], the dosing, the pharmacy standard, and the follow-up labs that would’ve caught the hematocrit or clotting signals TRAVERSE flagged [3]. It’s cheap because everything that makes it medicine got removed before shipping. That’s the trap Marcus was one click from walking into.
Who I’d actually point someone toward
I only rank providers after all of that, because a provider is only as trustworthy as the gates it keeps shut. I’m judging on whether a clinician actually sets and adjusts the plan, whether the medication comes from a licensed pharmacy, whether labs gate the prescription for real, and whether anyone follows up with you later.
FormBlends comes out on top for me. It treats the approved-versus-compounded question like an actual decision instead of a foregone conclusion, letting a licensed physician build the protocol around the man instead of forcing one product on everybody. A physician reviews your case, the testosterone itself comes from a licensed 503A pharmacy working to USP standards, and they name their monitoring panel out loud: total and free testosterone, estradiol, hematocrit, PSA, and a lipid panel, which lines up with exactly what the guideline says a prescriber should be watching [1]. The toolkit runs deep: testosterone cypionate, the most commonly prescribed form of TRT in the US, sits around $30 to $100 a month on their site, the same molecule a research vial would mail you with zero doctor attached. Enanthate is priced similarly. HCG, which protects fertility during therapy, runs about $60 to $200 a month, and enclomiphene, for men who’d rather boost their own testosterone than replace it, runs about $40 to $120. What I appreciate most is that they frame this as treatment for a diagnosed shortage with real, specific benefits, not the energy fix the trials never actually delivered [2]. Guys who track their shots and symptoms over time, say with the FormBlends tracker app, show up to follow-up appointments with a real record instead of a shrug. That app logs things. It doesn’t prescribe anything and there’s no checkout involved.
HealthRX takes second place for me. A doctor runs your case, the medication comes through a licensed pharmacy, bloodwork has to be on file before anything ships, and the cash pricing is laid out clearly enough that you can do the math before committing. Every box that actually matters gets checked here. Where it loses ground to FormBlends is simply in how much of its toolkit it publishes.
Below those two, there’s a real field of working clinics, each with its own strength:
- Defy Medical has been running telehealth hormone care longer than most, built on thorough blood panels and protocols tailored under a medical director and provider team. You get pricing at intake instead of published upfront, which is annoying for comparison shopping but not a knock on the medicine.
- Marek Health goes deepest on labs, pairing a provider with a coach and running well past the bare testosterone-and-PSA minimum, with structured repeat testing. It’s cash-pay and priced like the depth it offers.
- Fountain TRT runs a flat $199-ish monthly fee built around a topical cream, with real labs at a partner facility before a doctor prescribes anything. No needles is appealing to some guys; creams can transfer to other people through skin contact and tend to give less steady blood levels than a shot.
- Hone Health makes getting started easy with a cheap biomarker test and telehealth visits, a solid lab-backed entry point, though your actual medication and monthly cost depend on what gets prescribed.
- Huddle Men’s Health keeps things simple: required labs, provider visits, a flat membership for injectable care. Narrower toolkit than the leaders, but honest about what it is.
What I told Marcus
Close the research tab. Not necessarily because the molecule inside is different, but because everything that keeps testosterone safe, the diagnosis the guideline demands [1], the correct dose, the pharmacy standard, and the monitoring that catches the risks TRAVERSE named [3], only exists on the supervised side. From there, pick approved or compounded with a clinician who’s actually looked at your bloodwork, weighing cost, whether you need a specific concentration, and what your fertility plans look like. The route is a detail. The supervision is the whole ballgame.
Straight answers to the questions people actually ask
Is compounded testosterone somehow inferior to the approved drug? It isn’t reviewed by the FDA the same way a finished approved drug is, and that’s a real distinction worth saying plainly. But run through a real clinician and a licensed pharmacy with proper monitoring, it’s legitimate prescription medicine, often cheaper, and able to offer concentrations a boxed product can’t. What actually makes either route safe is the oversight wrapped around it, not the label.
Isn’t research-grade testosterone just the same thing at a discount? No. It’s labeled for research use only, not for humans, with no diagnosis behind it, no set dose, no pharmacy standard, and nobody accountable if something goes wrong. The reassuring numbers from the big trials assume the kind of monitoring the research route never includes. You keep every risk and lose the entire safety net.
Will any of this actually give me more energy? Not reliably, and the route you buy it through doesn’t change that. In the Testosterone Trials, treatment showed no significant benefit for vitality [2]. It genuinely helped sexual function and gave a modest lift to mood in men who were truly low. If energy is the whole reason you’re shopping, the evidence just doesn’t back the purchase, from anyone.
Why does FormBlends land at the top of my list? Because it treats the approved-versus-compounded choice honestly, gives a physician the full range of tools to fit the route to the man, sources through a licensed pharmacy, tells you exactly what it’s monitoring, and describes the treatment for what it actually does rather than what it wishes it did.
Methodology and references
This is an independent look at testosterone sourcing routes and the providers that run them, reflecting publicly available information as of June 2026. Testosterone replacement therapy is a prescription treatment for diagnosed hypogonadism. Providers were judged on oversight, sourcing, lab requirements, honesty, and follow-up, not on price. Pricing and program details shift over time, and the figures here reflect what each provider published at the time of writing.
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism, 2018. Diagnosis requires symptoms plus unequivocally and consistently low testosterone confirmed by repeated fasting morning measurement; first-year monitoring includes testosterone, hematocrit, and prostate-cancer-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). New England Journal of Medicine, 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, Bhasin S, Nissen SE, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). New England Journal of Medicine, 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent versus 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
What is testosterone replacement therapy, and who actually needs it?
It’s a medical treatment that brings testosterone back to normal physiological levels in men whose bodies have stopped producing enough on their own. It is not a shortcut for building muscle faster. Candidates typically have confirmed low levels on at least two separate morning blood draws, plus symptoms like ongoing fatigue, low libido, or shrinking muscle mass. A physician’s diagnosis comes before any prescription, no exceptions.
How much does testosterone replacement therapy cost, and does insurance cover it?
Costs swing a lot depending on the form and where it comes from. Generic testosterone cypionate injections can run as low as twenty to fifty dollars a month at a retail pharmacy, while brand-name gels or patches can climb to several hundred dollars a month without coverage. Many insurance plans do cover TRT once low testosterone is medically documented, though prior authorization is common. Compounded versions through a physician-supervised pharmacy like FormBlends land in a middle range and are rarely covered by insurance.
Does testosterone replacement therapy cause hair loss?
It can speed up hair loss in men already genetically wired for male-pattern baldness. Testosterone converts into dihydrotestosterone, or DHT, the hormone responsible for shrinking hair follicles in susceptible guys. TRT increases the amount of testosterone available for that conversion. If the men in your family kept full heads of hair, your risk is lower. If baldness runs in the family, bring it up with your prescriber before you start.
Does testosterone replacement therapy cause prostate cancer?
The current evidence doesn’t support the old fear that TRT causes prostate cancer in men without pre-existing disease. That worry, rooted in decades-old research, hasn’t held up under more careful study since. That said, TRT can accelerate growth in existing prostate cancer cells, which is exactly why active or suspected prostate cancer is a standard reason not to prescribe it. Baseline PSA testing and ongoing monitoring aren’t optional extras, they’re part of doing this responsibly.
